My research broadly focuses on mental health stigma and this Fellowship project explores mental health stigma via deliberate and automatic cognition processes. This project utilizes a concept association task (CAT) to capture how people implicitly associate various concepts with different health conditions. If you have ever taken a free implicit association test (IAT) online or during a work training to see if you have any implicit biases (e.g., implicitly associating men with science or people of color with violence)- it is a similar design: respondents quickly sort dozens of concepts pairs as “related” or “not related” and the task is designed to tap into automatic cognitive processes. For example, you would read instructions and then see the pair in Figure 1 below and quickly click the A or L key on your keyboard depending on if you perceive the two concepts as related. Two other concepts will then pop up on the screen to be sorted.
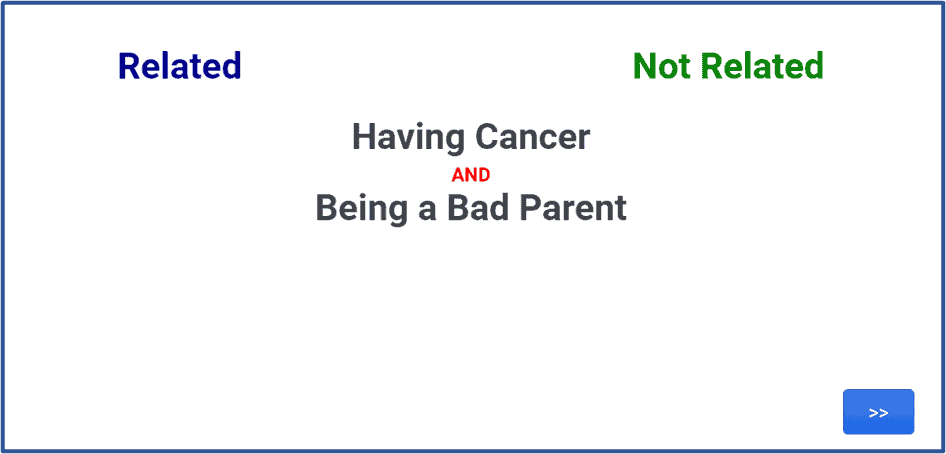
Figure 1. Concept Association Task Example
I was perhaps overly optimistic at the start of this project when I estimated how long finalizing the coding for the CAT and cleaning the data would take. But that is a lesson I have learned from seminar: projects take time and can evolve so patience, focus, and adaptability are key. I then moved on to re-familiarizing myself with the basics of R and learning more about data visualization tools in R, as well as reading about data visualization more generally. For example, Figure 2 displays a basic network visualization of a health schema creating from the CAT data. Each node represents a health condition (e.g., depression), social role (e.g., good/bad parent), causal attribution (e.g., due to genetics), or attribute/characteristic (e.g., being untrustworthy). Two nodes are connected when people implicitly associate the concepts as related (e.g., people associate schizophrenia with having bad character) and the color of that line signifies the strength of that association (e.g., red line indicates that people strongly associate schizophrenia with violence).
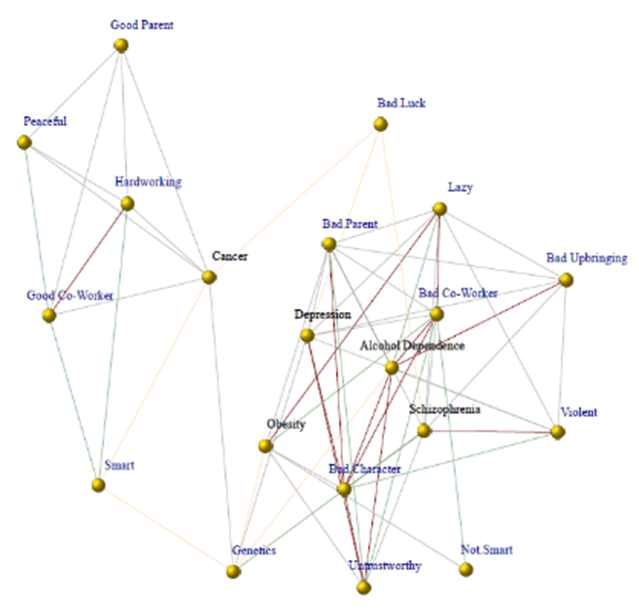
Figure 2. Basic network representation of health schemas
As the network visual displays, stigmatized health conditions may occupy different spaces in people’s mental maps compared to non-stigmatized health conditions. In other words, people implicitly sort certain concepts as “belonging” together, even if they are not aware of it. Unlike less stigmatized physical health conditions (e.g., cancer), mental health conditions (e.g., depression, schizophrenia, and alcohol dependence) may be implicitly grouped together with negative concepts (e.g., being a bad parent) and cognitively kept at a distance from more positive concepts (e.g, being a good co-worker).
The main goal of this Fellowship project is to illustrate mental health stigma through the juxtaposition of how people perceive mental health versus non-stigmatized physical health conditions. Some anti-stigma campaigns, such as the one displayed in Figure 3 below, have utilized this approach as a strategy to combat stigma.

Figure 3. Anti-stigma campaign using the “disease like any other” approach
These network representations aim to serve a similar purpose when coupled with information about mental health and the consequences of stigma (e.g., employment discrimination, social rejection, etc.). I am continuing to explore the most effective ways to present these findings to a public audience in an interactive, accessible way and my experience with the Digital Scholarship & Publishing Studio Fellowship has provided me with the tools and time to do so moving forward. As the Fellowship comes to an end, I realize I have much more to learn and look forward to the work ahead.
-Liz Felix